
Gaze is a complex action with multiple points of control and action. It is recommended that you learn and recap gaze control on the principles of neuro-ophthalmology page before reading further.
Internuclear Ophthalmoplegia (INO)
Internuclear refers to communication between CN6 (Pons) nucleus and the contralateral CN3 (midbrain) nucleus. This communication occurs via the medial longitudinal fasciculus (MLF). A lesion of the MLF results in internuclear ophthalmoplegia.
Normal MLF Function
Normally, the MLF coordinates the CN6 and CN3 to permit horizontal gaze.
- Recall that CN6 innervates the lateral rectus and CN3 innervates the medial rectus. The 2 muscles which are needed for horizontal gaze.
- The MLF connects the CN6 nucleus to the contralateral CN3 nucleus.
- e.g. the RIGHT MLF connects the LEFT CN6 nucleus to the RIGHT CN3.
Identifying The Lesion


- The lesion is made apparent on testing horizontal gaze.
- Unable to adduct the eye that is ipsilateral to the lesion (Ipsilateral CN3 function lost).
- Nystagmus on abduction of the contralateral eye (due to dissociation of vision).
i.e. for a RIGHT MLF lesion
- On attempted left gaze
- Unable to adduct right eye
- Abducting nystagmus of the left eye
- On attempted right gaze
- Normal movement
Bilateral INO (WEBINO/EBINO)
Bilateral internuclear ophthalmoplegia (INO) occurs when both MLFs are diseased. It is also called WEBINO or EBINO. 'WE' stands for wall-eyed in WEBINO. 'E' stands for Exotropic in 'EBINO'. WEBINO is an outdated term as it conveys a negative image.
Findings
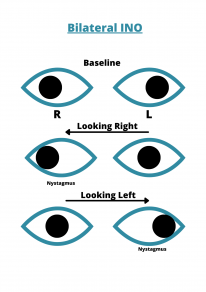
In the primary position, both eyes are slightly deviated outwards, hence wall-eyed/exotropic.
- On attempted LEFT gaze
- abducting nystagmus of the LEFT eye
- unable to adduct the RIGHT eye
- On attempted RIGHT gaze
- abducting nystagmus of the RIGHT eye
- unable to adduct LEFT eye
One and Half Syndrome
The ‘one’ refers to horizontal gaze palsy. This is caused by a lesion of the CN6 nucleus/PPRF. For example, a RIGHT CN6 nucleus lesion will stop the function of the right CN6 and the LEFT MLF. This means that neither eye will move on attempted RIGHT gaze. But LEFT gaze would be completely normal.
The 'half' refers to INO.
Findings

The eye which is ipsilateral to the lesion cannot abduct or adduct, and the contralateral eye can only abduct.
For RIGHT CN6/PPRF Lesion (ONE)
In the primary position, the right eye is deviated inwards, and the left eye is normal.
- On attempted right gaze
- Right eye will not move
- Left eye will not move (no impulse going down the MLF because it is broken at the CN6 nucleus)
- On attempted left gaze
- Normal movements (because the RIGHT CN6/PPRF only supplies the RIGHT lateral rectus and LEFT medial rectus (via CN3), neither of which are involved in horizontal gaze to the left)
For RIGHT INO (HALF)
- On attempted RIGHT gaze
- Normal movements
- On attempted LEFT gaze
- Abducting nystagmus of the LEFT eye
- Unable to adduct RIGHT eye
In RIGHT sided One and Half Syndrome (both of the above combined)
- In the primary position, the left eye is deviating outwards, and the right eye is in normal position (both the medial and lateral recti of the right eye are dysfunctional)
- On attempted right gaze
- Right eye will not move
- Left eye will not move
- On attempted left gaze
- Left eye abducts
- Right eye will not move
The Pontine paramedian reticular formation (PPRF) and the CN6 nucleus are separate entities but are very closely associated, and can be considered as one entity for this section.
Other Gaze abnormalities
Parinaud syndrome
A supranuclear palsy of upgaze. It is caused by a lesion in the dorsal midbrain.
Signs
- Bilateral lid retraction - Collier sign
- Upgaze paresis
- Convergence retraction nystagmus
- Large pupil with light-near dissociation (light reflex lost but near accommodation reflex intact)
Progressive Supranuclear Palsy
This one is easiest to spot because the vignette will demonstrate classic Parkinsonian signs.
- Parkinsonism, postural instability and vertical gaze palsy
- Axial rigidity and poor response to levodopa