The term 'primary' is used to describe idiopathic/isolated disease, where no precipitating trigger has been found. The term 'glaucoma' is used to describe characteristic optic disc changes alongside visual field defects. Therefore, 'primary glaucoma' refers to idiopathic/isolated optic disc changes and corresponding visual field defects. Primary glaucoma is further classified according to the state of the anterior chamber (AC) angle: open or closed.
Primary Open Angle Glaucoma (POAG)
Chronic glaucomatous change due to optic nerve damage with an open anterior chamber angle.
Pathology
This is a 'primary' disease, meaning there is no identifiable cause of the glaucomatous change.
Risk Factors
MYOC and OPTN gene mutations.
Steroids.
Smoking.
Myopia.
Afro-Caribbean race.
Increasing age.
People of Afro-Caribbean origin are more likely to be myopic (longer eyes) and are at risk of open-angle glaucoma, compared to east Asians who are more likely to be hyperopic (shorter eyes) and at risk of angle-closure glaucoma.
Diagnostics
Presentation
Asymptomatic at first but will develop visual field defects.
Typical presentation is a 60-year-old black myope with a history of vascular risk factors.
Investigations
Tonometry: IOP > 21mmHg.
Slit-lamp examination: no signs of precipitating diseases.
Gonioscopy: open angle.
Fundoscopy: glaucomatous optic disc changes.
Perimetry: visual field defects.
Management
Treatment aims to control IOP.
Topical IOP lowering medications (1st line)
Topical prostaglandin or beta-blocker (other options are alpha-2 agonists, and carbonic anhydrase inhibitors).
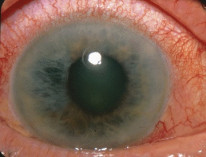
Primary angle-closure glaucoma: ITC + Glaucomatous damage + elevated IOP or PAS or APAC episodes Acute angle-closure of the right eye. By James Heilman, MD, CC BY-SA 3.0
Pathology
Pupil block mechanism (Majority):
Apposition of iris to lens → abnormal aqueous flow through the pupil → increase in the pressure difference between the posterior and anterior chambers → anterior bowing of the peripheral iris leading → peripheral anterior synechiae (PAS) → angle closure → obstructed aqueous outflow → elevated IOP → glaucomatous optic nerve damage
Sudden Pain + blurred vision + nausea + worse in the dark + red eye An eye with acute angle closure. The pupil is irregular and mid dilated. The eye is red and the cornea is hazy. By Jonathan Trobe, M.D., CC BY 3.0, via Wikimedia Commons.
Episodes of APAC or same as APAC but with glaucomatous changes.
A more chronic state of disease.
Investigations
Tonometry: IOP>21mmHg.
Gonioscopy: closed-angle.
A closed-angle on gonioscopy is indicative of angle closure. To diagnose angle-closure glaucoma, you must see glaucomatous optic disc changes and visual field defects.
Management
APAC
The aim is to stabilize IOP quickly to prevent blindness.
Monitor and consider systemic hyperosmotics (IV mannitol).
Definitive treatment is bilateral peripheral iridotomy, with either ND:YAG laser or surgery.
PACG
The aim is to control IOP over time.
Bilateral peripheral iridotomy.
The same medication protocol as POAG.
Cataract extraction is effective in acute and chronic stages.
Peripheral iridotomy is done bilaterally because angle closure in one eye drastically increases the risk of angle-closure in the fellow eye (other eye).
Primary Congenital Glaucoma
Glaucoma in the first year of life due to malformed anterior chamber angles.
Pathology
Mostly sporadic but can be autosomal recessive.
CYP1B1 gene mutation association.
Diagnostics
Presentation
Hx: infant boy + haab striae + buphthalmos + large corneal diameter + epiphora.
Investigation
Elevated IOP (normal in infants is 10–12 mmHg).
Widened corneal diameter.
Management
Angle surgery: Goniotomy if the cornea is clear. If the cornea is cloudy, then trabeculectomy can be attempted.
Normal Tension Glaucoma (NTG)
NTG is POAG with persistently normal IOP (≤21 mmHg).
Pathology
Glaucomatous changes with normal IOP.
Risk factors for progression
Female sex.
History of migraine.
Disc haemorrhage at diagnosis.
Diagnostics
Presentation
Asymptomatic.
More common in elderly east Asian females.
Symptoms of vascular dysregulation such as migraine, Raynaud's, and low BP.
Investigations
Tonometry: normal IOP.
Gonioscopy: open angle.
Fundoscopy: optic disc changes.
Perimetry: visual field defects.
Treatment follows the same protocol as POAG.
Tonometry can be falsely low in people with thinner corneas. This can be picked up with pachymetry.
Ocular Hypertension (OHT)
Raised IOP (>21 mmHg) without glaucomatous damage.
Summary
Some OHT patients convert to primary open-angle glaucoma within several years.