
Inflammation of the orbit can be painful and sight-threatening. This page reviews the important causes of orbital inflammation.
Cellulitis (Orbital and Preseptal)
Orbital and preseptal cellulitis are important diseases that must be distinguished in the clinic. Orbital cellulitis is severe and preseptal cellulitis is mild.

Preseptal |
Orbital |
|---|---|
Infection anterior to the orbital septum. |
Infection of the eye socket behind the orbital septum. |
Typically caused by direct infection from lid trauma, by Staphylococcus aureus. |
Typically caused by infection via air sinuses (ethmoid sinus) by Streptococcus pneumoniae and Haemophilus influenzae. |
Patients present with lid inflammation and low-grade fever, and no signs of eye involvement. |
Commonly affects children, who present with an acutely inflamed orbit, proptosis, fever, restricted ocular movements, defects in vision and Relative Afferent Pupillary Defect (RAPD). |
Treatment → PO antibiotics. |
Can be severe and progress into the brain. The patient is admitted and treated with IV antibiotics. |
Preseptal vs Orbital(Postseptal) is anatomically demarcated by the orbital septum which is a membrane that extends from the orbital rim and inserts into the eyelids. CT of the orbit confirms the diagnosis.
Thyroid Eye Disease (TED)
TED is the most common cause of axial proptosis in adults. It is also commonly tested during the exam.
Pathology
Stages
- An active inflammatory stage in which the eyes are red and painful.
- Followed by a fibrotic phase involving the extraocular muscles where there is oedema and fibrosis. This leads to restrictive myopathy, exophthalmos and optic neuropathy.
Pathomechanism
- TSH IgG binds to TSHr on extraocular muscles and fibroblasts → leads to adipogenesis and hyaluronic acid deposition in orbital muscle → leads to swelling of muscles and fat.
- Lid retraction occurs due to the sympathetic overstimulation of Müller's muscle.
Diagnostics
Presentation
- Most important risk factor is smoking.
- Patients are typically hyperthyroid but can be eu/hypothyroid.
- Axial proptosis.
- Lid retraction (Dalrymple sign) - occurs due to sympathetic overstimulation of Müller's muscle, driven by elevated thyroid hormone.
- Lid lag (Von Graefe sign).
- Characteristic staring appearance (Kocher sign).
- Restrictive myopathy typically affects the inferior rectus first.
- Half the patients with superior limbic keratoconjunctivitis also have TED.
Investigations
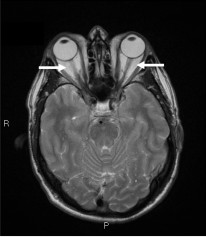
- CT of the orbit characteristically shows thickening of extraocular/levator muscle and sparing of the tendons.
- Anti-TSHr antibody.
If there are signs of optic neuropathy (dyschromatopsia, RAPD, field and acuity defects) urgent anti-inflammatory treatment is needed to prevent vision loss.
Management
Severe/acute (myopathy or significant clinical findings or optic neuropathy)
- IV methylprednisolone followed by oral prednisolone.
- If steroids are contraindicated, orbital radiation can be used.
Mild/Chronic
- Aim for euthyroid in all patients.
- Lubricants.
- Taping (tape the eyelid shut overnight to minimise exposure keratopathy).
- Topical Cyclosporine to reduce inflammation.
Fibrotic phase
- Orbital decompression surgery can be offered during the fibrotic phase to address exophthalmos.
Stopping smoking is the most important step in chronic management.
Other Causes of Orbital Inflammation
Description |
Key Features |
|
|---|---|---|
Tolosa-Hunt syndrome (Superior orbital fissure syndrome; Cavernous sinus syndrome; Cavernous sinus granulomatosis) |
A syndrome of headache, ophthalmoplegia and periorbital sensory loss. Caused by granulomatous inflammation of the orbit, cavernous sinus or superior orbital fissure. |
|
Granulomatosis with polyangiitis (Wegener's granulomatosis) |
A multisystem necrotising vasculitis that typically affects the upper respiratory tract, kidneys and lungs. |
|
Sarcoidosis |
A multisystem noncaseating granulomatous disorder that manifests in the eye as uveitis. |
|
Diagnosis of Tolosa-Hunt is made by correlating the signs and symptoms with granulomatous inflammation demonstrated by MRI/biopsy.